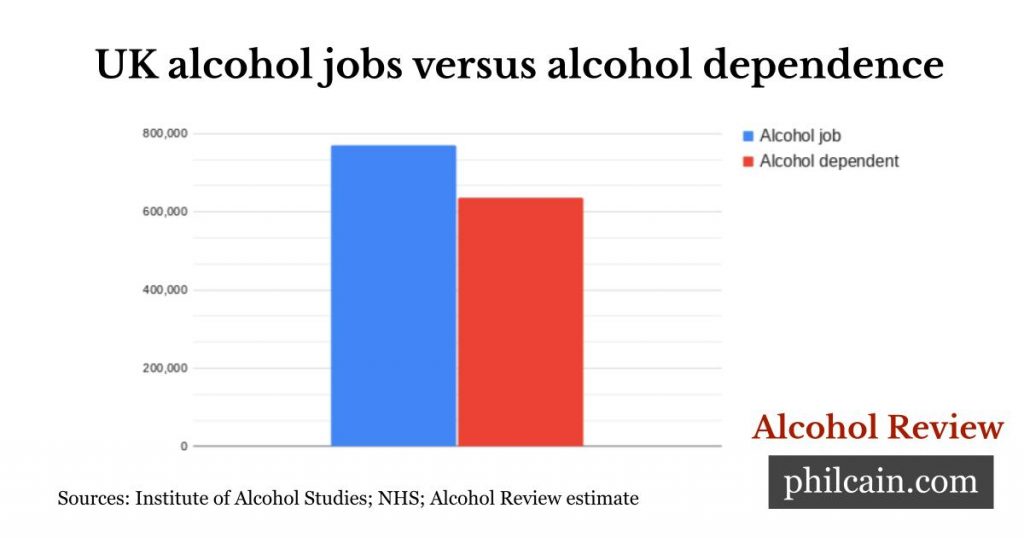
There are maybe 770,000 part-time and full-time jobs connected with alcohol business in the UK, according to an IAS estimate. And there are about 638.000 people who are alcohol dependent, meaning they experience side effects when not inebriated. ■
Alcohol understanding for all
There are maybe 770,000 part-time and full-time jobs connected with alcohol business in the UK, according to an IAS estimate. And there are about 638.000 people who are alcohol dependent, meaning they experience side effects when not inebriated. ■
by Nicole Lee, Curtin University
With everything going on over the past couple of years, many people have changed their drinking habits.
We’ve seen an increased demand for support, suggesting more people are trying to cut back or quit.
There are so many options for cutting back or quitting alcohol it’s hard to know what will be most effective.
What works depends on how much you drink
Most people successfully quit or cut back their alcohol consumption on their own.
People who drink more frequently are much more likely to have symptoms of dependence and might find it more difficult.
You might be dependent if:
The more of these signs you have and the more severe they are, the more dependent you’re likely to be. You can check your risk of dependence here.
If you have a mild dependence on alcohol, you may be able to cut back on your own. But if you are moderately dependent, you may need to get some kind of support.
If you are severely dependent, you should seek medical advice before you make any change to your drinking because stopping suddenly can cause severe health problems, including seizures and even death in some people.
For people who are severely dependent, the usual recommendation is to take a permanent or temporary break from alcohol. It may take six months to a year or more before you are able to start drinking again. Some people find it’s better for them not to drink again at all. With severe dependence, there’s a high risk of quickly going back to heavy drinking if you just try to cut back.
If you experience any symptoms of dependence, once you stop or cut back your drinking, you might need specialist treatment or ongoing support to prevent going back to heavy drinking.
‘Cold turkey’ or reduction?
If you’re not dependent, you should be able to either reduce the quantity or frequency of drinking or quit altogether. You may do this on your own or choose to get some support. If one method doesn’t work, try a different way.
If you experience mild to moderate dependence, every time you have a drink it can become a trigger to drink more. So it’s sometimes easier to increase drink-free days, rather than reducing the quantity on drinking days, or to quit altogether for a period of time.
People who are severely dependent usually require some kind of withdrawal support to stop drinking. It is usually better to stop altogether (“cold turkey”) as long as you have medical support. You can undertake withdrawal treatment in a hospital, at home with the help of a GP or nurse, or via telehealth. Alcohol withdrawal typically lasts about five to seven days.
Zero-alcohol drinks
Zero-alcohol drinks are alcoholic drinks with the alcohol removed but which retain a taste similar to the alcoholic version. There is now a huge variety of options for spirits, beer and wine.
If you are not dependent but are trying to reduce your alcohol intake for health or other reasons, these can be a good option. By replacing some or all of your usual alcoholic drinks with zero-alcohol drinks, you can still enjoy the social aspects of drinking without the health risks of alcohol.
If you are dependent on alcohol, the smell and taste of zero-alcohol drinks can act as a trigger for drinking alcohol. They might make it more difficult to make permanent changes to your drinking.
Treatment apps and online support
A range of computerised, web-based, and mobile apps have been developed to support people cutting back or quitting alcohol. They have shown promising results in early trials. The benefit of these apps is accessibility, but the outcomes are modest and they seem to work best in conjunction with professional support.
Hello Sunday Morning’s Daybreak program is a large online alcohol support community, accessed through a mobile and desktop app. It’s designed for moderate drinkers who want to cut back or quit. Early research suggests it’s effective in reducing drinking, as well as improving psychological well-being and quality of life.
Some previously face-to-face support groups like SMART Recovery and Alcoholics Anonymous have moved online, which has increased accessibility. These are typically more suited to people who are dependent on alcohol.
Psychological interventions
Brief interventions: As little as five minutes of advice from a GP can reduce alcohol consumption by 30%, especially for people who are in the mild to moderate dependence category. So it’s worth chatting to your doctor if you need a little help getting started.
Counselling and psychological therapy: The main treatment type to help with alcohol issues is counselling. Sessions are usually once a week with a qualified professional, such as a psychologist. Sometimes they are delivered in group settings. Counselling is suitable for any level of drinker who is trying to make changes.
Some of the main evidence-based counselling treatments in Australia are behavioural and cognitive therapies, such as cognitive behavioural therapy and mindfulness-based relapse prevention. These types of treatments have been shown to be at least as effective as medication
Intensive group programs
A number of more intensive group programs are suited to people who are dependent on alcohol or who are having significant problems, including:
Medication
A number of medications can help people who are moderately to severely dependent on alcohol. They tend to work best in conjunction with counselling.
Self-help groups
Alcoholics Anonymous’s 12-step movement has a long history dating back to the 1930s, when there was very little available in the way of real alcohol treatment. There is relatively little research on AA and much of that has been conducted from within the organisation. The known outcomes are modest – the success rate is estimated to be around 10% and the dropout rate appears high.
AA can be helpful for some people and also provides a very well-established peer support network if you need support. It seems to be more effective in conjunction with professional treatment.
There are many options if you are trying to reduce your drinking and no single strategy works for everyone. The best approach is to start with something that looks appealing and feasible to get the outcomes you are looking for. If that’s not effective, try something else or seek professional help.![]() ■
■
Nicole Lee, Professor at the National Drug Research Institute (Melbourne), Curtin University
This article is republished from The Conversation under a Creative Commons license. Read the original article.

The heaviest drinking households bought 17 times more alcohol than the lightest drinking ones at the start of the covid pandemic, a study says, helping to explain record high levels of alcohol-induced death.
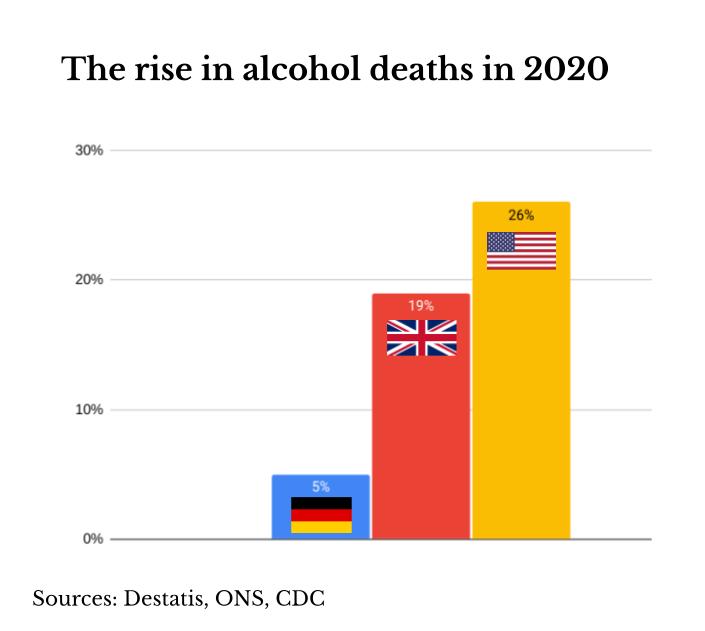
The polarisation of alcohol consumption found between the top and bottom fifth of households in the UK is likely one reason why there was a 19% rise in alcohol-specific deaths in 2020, reaching the highest level for 20 years.
The US saw an even bigger alcohol-induced death surge in 2020 Alcohol Review revealed last month (see chart). The CDC has since confirmed the 26% rise that year and now also estimates a similarly high level for last year.
The increase in US deaths has so far attracted scant public attention or research. But it is likely the lifestyle changes and stress of the covid crisis saw heavier drinkers in both sides of the Atlantic increase their intake to deadly levels, just as this research suggests they did in the opening phase of the covid crisis in the UK.
Late last year around 30% more people in England said they drank more than the official low risk guidelines of 14 units (140ml) a week compared to before the covid crisis, said a Office for Health Improvement and Disparities survey.
“It is also likely that reduced access to care and treatment during covid contributed to an increase in alcohol-related deaths,” said lead author Professor Peter Anderson of Newcastle University when asked if other factors played a part in the UK.
Households in the more socially disadvantaged locations of northern England bought more alcohol. The pattern in Scotland and Wales was “less pronounced”, possibly because they have minimum alcohol pricing policies, the study says.
“This suggests that a focus on policies to reduce high levels of drinking are even more important in extraordinary times, such as those we’ve seen since March 2020,” said Professor Anderson from Newcastle University.
“By failing to implement minimum unit pricing as part of its plans for public health, England is now falling further behind the rest of the UK in the race to tackle alcohol harm,” said Professor Sir Ian Gilmore of the Alcohol Health Alliance.
The research is a joint project between Newcastle University and the National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) North East and North Cumbria.
The study used retail data from Kantar WorldPanel for 30,000 UK homes for six years to 2020. ■

Increasing our exposure to an activity, like say playing piano, typically increases our skills in that activity, but the opposite is the case with alcohol drinking because it is an addictive psychoactive. The negative effects of exposure are greatest when we are still young and our brains are still forming. Find out more. ■

Alcohol is not useful, with all of its purported benefits achievable by other means which are not hazardous to health or well-being. Please join the supporters of Alcohol Review to help bring alcohol understanding for all. ■

Children and people having difficulties with alcohol should be spared from a “constant bombardment” of alcohol advertising, say health experts with the backing of MPs.
The group describes it as “bizarre” alcohol is not part of the Health and Care Bill, which is meant to introduce advertising restrictions such as a 9pm watershed for ‘less healthy food or drink’ from the end of next year.
“With deaths linked to alcohol at record highs, we are in desperate need of a new approach,” said Professor Sir Ian Gilmore, who heads the Alcohol Health Alliance, which represents over 60 NGOs.
The call comes with the release of a report highlighting how alcohol marketing can be problematic for vulnerable groups, such as those in recovery being a ‘trigger’ for relapse. It says the UK should fall into line with the WHO recommendation to restrict alcohol marketing.
The intense alcohol marketing of alcohol over Christmas and at sports events, makes it difficult for those in active addiction and recovery to fully participate in everyday life, they say.
Speaking at the report launch, Melissa Rice, who is in recovery, asked attendees to imagine the difficulties that might arise if Gogglebox was sponsored by cocaine.
MPs backing the call include Conservatives Christian Wakeford, chair of a parliamentary committee on alcohol harm and the Labour vice-chair, Dan Carden.
They also include Alex Norris, Labour’s Shadow Public Health Secretary, and Conservative Derek Thomas, Commissioner for Alcohol Harm. ■