
The heaviest drinking households bought 17 times more alcohol than the lightest drinking ones at the start of the covid pandemic, a study says, helping to explain record high levels of alcohol-induced death.
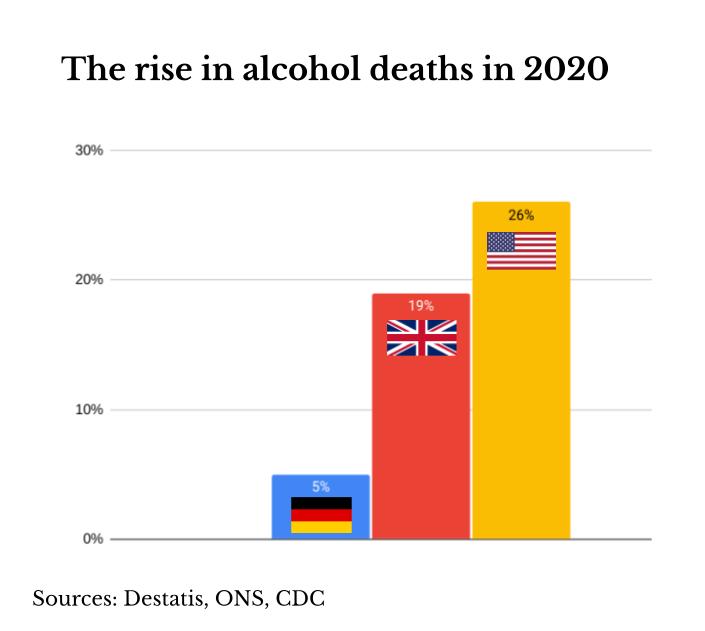
The polarisation of alcohol consumption found between the top and bottom fifth of households in the UK is likely one reason why there was a 19% rise in alcohol-specific deaths in 2020, reaching the highest level for 20 years.
The US saw an even bigger alcohol-induced death surge in 2020 Alcohol Review revealed last month (see chart). The CDC has since confirmed the 26% rise that year and now also estimates a similarly high level for last year.
The increase in US deaths has so far attracted scant public attention or research. But it is likely the lifestyle changes and stress of the covid crisis saw heavier drinkers in both sides of the Atlantic increase their intake to deadly levels, just as this research suggests they did in the opening phase of the covid crisis in the UK.
Late last year around 30% more people in England said they drank more than the official low risk guidelines of 14 units (140ml) a week compared to before the covid crisis, said a Office for Health Improvement and Disparities survey.
“It is also likely that reduced access to care and treatment during covid contributed to an increase in alcohol-related deaths,” said lead author Professor Peter Anderson of Newcastle University when asked if other factors played a part in the UK.
Households in the more socially disadvantaged locations of northern England bought more alcohol. The pattern in Scotland and Wales was “less pronounced”, possibly because they have minimum alcohol pricing policies, the study says.
“This suggests that a focus on policies to reduce high levels of drinking are even more important in extraordinary times, such as those we’ve seen since March 2020,” said Professor Anderson from Newcastle University.
“By failing to implement minimum unit pricing as part of its plans for public health, England is now falling further behind the rest of the UK in the race to tackle alcohol harm,” said Professor Sir Ian Gilmore of the Alcohol Health Alliance.
The research is a joint project between Newcastle University and the National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) North East and North Cumbria.
The study used retail data from Kantar WorldPanel for 30,000 UK homes for six years to 2020. ■








{kind=link}