
Make your own: Alcohol-free vodka
Alcohol understanding for all
Find this service useful?
Please join the Alcohol Review‘s supporters who make it possible

*Subscribe *Books *Whatsapp *Twitter, LinkedIn *ARchive
In this issue: Olympics strikes first global beer deal; Local alcohol levies mooted; Pope issues wine reminder; Smaller glasses cut drinking; US alcohol deaths state-by-state; and more
Olympic beer deal: The Olympics’ first ever global beer promotion deal drew sharp criticism from a range of UK health advocates, including the Association of Directors of Public Health. The deal to promote beer brands at the next two Olympics covers all brands in AB InBev’s portfolio, Alcohol Review was told. The Olympics organiser said the beer branding will not be seen in the field of play and will initially revolve around the Corona Cero alcohol-free brand, a modified version of the 4.5% brand. At the LA games in 2028 the emphasis will switch to the 3.5% Michelob Ultra brand, marketed as low calorie.
Local levies: Local levies on alcohol and other unhealthy products could raise funds and reduce inequality, said the left-leaning UK think tank IPPR in a new report. Such levies would top up £3bn funding from a Health Creation Fund, with poorer areas where unhealthy outlets cluster able to raise more money. Scottish Labour said earlier in the month that it is backing an alcohol levy.
Papal whine: Pope Francis was reported to have reminded Italian wine producers of their moral and ethical responsibilities, while reassuring them their product is a “gift from God”. His reminder may relate to the Italian industry being at the vanguard of resistance to nutrition and ingredients labels.
Glass ceiling: A study removing the largest glass of wine from sale in pubs cut the total amount of alcohol consumed by 7.6%, while income remained the same. One commentator suggested huge glasses are naff anyway, while another felt the discussion was a sure sign a full ban on alcohol is nigh.
US deaths state-by-state: Alcohol Review published a table of rises in US alcohol-induced deaths by state, using provisional CDC figures. They range from Mississippi with an 85% rise and New Jersey with 11%. PBS this month talked to the author of a new four-part series in the Denver Post on how alcohol has not been treated with the same urgency as opioids. Colorado, the CDC data says, is in the middle with a 32% in deaths.
Conflicted again: The US organisation assembling a committee to assess evidence for an update to alcohol guidelines has picked a Harvard professor with financial ties to the alcohol industry, having recently backtracked on the appointment of two people with such ties.
AI ageing: The UK government is considering the use of age assurance technologies, including age estimation to decide if an individual is old enough to purchase age restricted products like alcohol.
Alcohol share prices in the US are far stronger than before the covid-19 slump struck with the US Alcoholic Beverages/Drinks Index up a fifth over the full year, having almost halved in February (see chart).
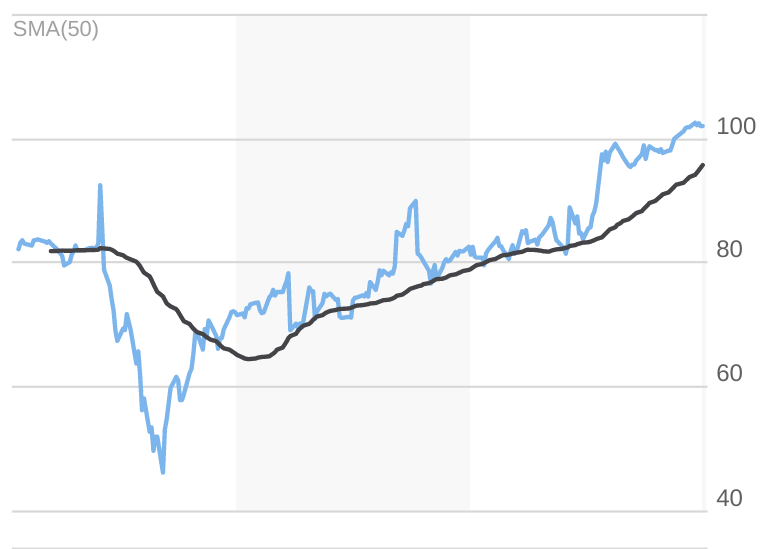
A share price rise needn’t necessarily indicate an expectation of higher profits or revenue. It could be a “flight to safety”, where people make more reliable bets in crises, which is why gold prices go up.
Interpreting share movements is a matter of speculation. This interpretation would indicate the US financial market expects alcohol to fair relatively well and is willing to bank on it. ■
UK release, July 2nd; certificate 12A
I hoped Another Round, an international Oscar winner about alcohol, might at least be entertaining, despite some obvious flaws. But I was disappointed.
I am no film critic, but I believe etiquette demands some positives at this point. The film is well made, well acted and shot, and there are moments of real pathos and extended periods of the bleak sadness that Scandinavia is so good at.
The lasting sadness, however, is that all this undoubted artistic skill and talent was employed in exploring alcohol through an idea even its own supposed inventor, psychiatrist Finn Skarderud, says was no more than an offhand joke.
There is also a Smirnoff vodka bottle put in the hands of photogenic lead actor Mads Mikkelsen, who just happens to also be the face of brewer Carlsberg. It is hard to imagine either appear accidentally or without conditions attached.
The premise is, some tell me, not even an original joke, but an oft-repeated psychiatrists’ common room gag, made funny mainly because it is obvious nonsense. The idea is, I should say, we are born with a deficit of 0.05% of alcohol in our blood.
The film cracks on, nonetheless, making this patently phoney idea its intellectual cornerstone. The audience is thereby invited to suspend their disbelief for a large chunk of a rather plodding 2.5 hours of image after image superficially “proving” the theory.
And for about two-thirds of the film things go swimmingly. Four grouchy middle-aged Danish men start teaching tiddly, perform like champs and generally regain their lost mojo. “All fired up and relaxed at the same time,” as one puts it.
Predictably, enough, they up the dose. But only after they reach more than double the 0.05% “deficit” does it go horribly wrong. No matter that it is a daft idea to depend on alcohol to do your job from the start, particularly if you look after kids.
But it is good, one might argue, that the film goes on to disproves its own crackpot theory in the tragic ending. Well, it does, sure, but [unapologetic spoiler] a few shots later alcohol is the catalyst of the final euphoric scene.
The film also does things like making Churchill’s notorious heavy drinking an unarguable endorsement of a liberating habit. It also fails to mention that Ernest Hemmingway’s alcohol drinking was life threatening for decades. Yada yada.
“Misuse of drugs must be infrequent and should not be glamorised or give detailed instruction,” is among the conditions of the UK’s 12A certificate, and films must not promote dangerous or anti-social behaviour.
There is a tragedy, sadness and a bit of sanitised puking, but these do not outweigh the impression left by the far longer sections in which we watch male role models experience a quasi-scientific miracle, reprised at the end.
In the closing scene Mikkelsen’s dour history teacher has a post-funeral pick-me-up enabling him to dance with the kids like it was 1999, before flinging himself fully-clothed off a jetty in a final alcohol-fuelled flourish.
There is a great film to be made about alcohol, about its real effects, dramas, humour, confusions and contradictions. This, sadly, is not it, and despite its many troubling flaws it seems likely to fill the niche for years to come. ■
A decade ago, while working in a women’s prison, I met a young woman whose story would leave an indelible mark on me. She had endured severe abuse at the hands of men, and I was initially concerned that, as a male social worker, my presence might rekindle her trauma. Yet, through careful and considered engagement, we were able to forge a relationship of trust.
Jenny* confided in me that heroin had become her refuge – the only respite that quieted the relentless storm of her thoughts. But her dependency had brought dire consequences: the removal of her children and her subsequent imprisonment for possession with intent to supply. Even so, Jenny told me that before she was imprisoned: “Heroin was the only thing that helped me to cope.”
While inside, she experienced regular flashbacks and profound anxiety. Her treatment regime included antipsychotic medication Seroquel and heroin replacement Subutex – but Jenny didn’t use them conventionally. “The only way they help is if I grind them together and snort them,” she explained. This method provided her a fleeting, euphoric respite from her psychological torment.
Across the world, we’re seeing unprecedented levels of mental illness at all ages, from children to the very old – with huge costs to families, communities and economies. In this series, we investigate what’s causing this crisis, and report on the latest research to improve people’s mental health at all stages of life.
It wasn’t Jenny’s drug revelation that struck me most profoundly, but the reaction of some of my prison colleagues. Her unconventional use of the medication was labelled substance abuse, leading to her being ostracised by the prison’s mental health service, which refused to work with her until she “sorted out” her drug issues.
Even though I had known Jenny for a year, it was only when she was about to be released from prison that I really understood how serious her situation was. I was shocked to see her breaking the prison’s rules on purpose because she didn’t want to leave. She started smoking in places she shouldn’t, damaged her own cell and areas everyone used, attacked another prisoner, which was not like her at all, and started using spice and hooch.
Jenny preferred staying in jail over facing life outside, but she was let out all the same. A week after her release, I received news that she had died from a heroin overdose.
Mental health problems are experienced by the majority of drug and alcohol users in community substance use treatment. Death by suicide is also common, with a history of alcohol or drug use being recorded in 54% of all suicides in people experiencing mental health problems. (Public Health England guide
, 2017.)
Jenny’s tragic story left me with many questions – what were the underlying causes of mental illness? What spurred the spiral into addiction? Why did individuals turn to substance use? – that, even after six years as a mental health social worker working in prisons and psychiatric hospitals, I had neither the knowledge nor experience to answer. Talking to colleagues did not resolve them, so I sought answers by returning to academia alongside my day job.
A postgraduate diploma helped me better understand the theories of mental health from neuroscientific, psychiatric and pharmacological perspectives. But above all, I realised that many of the people I was now encountering in my new role, working in a crisis home treatment team (a community-based team set up to support people experiencing severe mental health issues), would never get better. Rather, they would just keep coming back with a new crisis.
And for a large majority of them (around four in five), substances ranging from highly addictive narcotics to potent, mind-altering chemicals would be a key part of their daily lives in addition to, or as an alternative for, their prescribed psychiatric medication..
Roger was one of many people I met who relied on Spice, a synthetic cannabinoid designed to mimic the effects of naturally occurring THC. (In addition to consumption by smoking, there are increasing reports of synthetic cannabinoids being used in e-cigarettes or vapes.)
Nonetheless, Roger told me Spice was the “only thing that would help sort my head out”. And, after listening to a lecture from me about the dangers of these substances, he responded:
I know how much to take – I know when I’ve taken too much or not enough. I use it in doses now. Why would I stop if it’s the only thing that works?
It was clear that Roger knew much more about the effects of Spice than I did. Interactions like this ignited a desire in me for deeper knowledge – not from books or universities, but directly from people with co-existing mental health and addiction problems.
Perhaps surprisingly, in the UK we don’t know how many people are living in this combined state. Estimates have tended to focus only on people with severe mental health problems and problematic substance use. For example, a 2002 Department of Health guide suggested that 8-15% of its patients had a dual diagnosis – while acknowledging that it is difficult to assess exact levels of substance use, both in the general population and among those with mental health problems.
A decade earlier, US research had identified that for people with schizophrenia, substance use (non-prescribed drugs) was a significant problem relative to the general population. More recently, a 2023 global review of evidence identified that the prevalence of co-existing mental health and substance use among children and adolescents treated for psychiatric conditions ranged between 18.3% and 54%.

But what I found particularly interesting was an analysis of the writings of Thomas De Quincey from more than 200 years ago. In his 2009 article Lessons From an English Opium Eater: Thomas De Quincey Reconsidered, leading clinical academic, John Strang, highlighted that issues raised by De Quincey in 1821 remain causes for concern some two centuries later.
De Quincey was arguably the first person to document his own use of substances, in particular opium. His writing shows that he self-medicated to manage pain, including “excruciating rheumatic pains of the head and face”:
It was not for the purpose of creating pleasure, but of mitigating pain in the severest degree, that I first began to use opium as an article of daily diet … In an hour, oh Heavens! What an upheaving, from its lowest depths, of the inner spirit!
De Quincey’s use of non-prescribed drugs mirrors that of John, Jenny, Roger and so many other people I have met as a social worker. Clearly, we’ve known about the close relationship between mental illness and substance abuse for hundreds of years, yet are still wrestling with how best to respond.
Official guidance almost always advocates for a “no wrong door” policy![]()
![]()
![]()
![]() , meaning that those with dual addiction and mental health issues will get help whichever service encounters them first. But from what people with lived experience were telling me, this was not the case.
, meaning that those with dual addiction and mental health issues will get help whichever service encounters them first. But from what people with lived experience were telling me, this was not the case.
I sent freedom of information requests to 54 mental health trusts across England, to try to discern any patterns of variation in the way their patients were being measured and treated. Some 90% of the trusts responded, of which a majority (58%) recognised the dual occurrence of mental illness and substance use. However, the estimated prevalence of this dual diagnosis varied widely – from only nine to around 1,200 patients per trust.
What I found most alarming was that less than 30% of the mental health trusts said they have a specialised service for addiction which accepts referrals for dual diagnosis patients. In other words, throughout England, a lot of these patients are not being appropriately supported.

I started using when I was around 18. Things weren’t good in my life at the time, and I got in with a crowd who offered me heroin. It was the most amazing experience; all my worries disappeared better than the antidepressants I had been taking. But the more I used, the more I needed it. Now I use it in stages, just before I go to work and at night.
Carl had been using heroin for more than ten years when I interviewed him. When I asked if he wanted to stop, he shrugged and said no, explaining:
I’ve tried so many times – I’ve been on methadone but that was worse, especially coming off it. I know how much to take, and no one knows I use gear – so, no. But, as soon as you tell a professional you take heroin, their whole attitude changes. I’ve seen it many times. I dress quite well and I have a job, but as soon as I say I use heroin, they change. It’s almost as if they don’t see the same person any more.
Talking to Carl underlined that many users know far more than me about the substances they take and why they take them. Yet as soon as a professional (typically a nurse, social worker or doctor) hears they are taking an illegal substance, or are misusing a legal substance such as alcohol, they are stigmatised and often ostracised from service provision.
Suzanne was homeless and also using heroin, but for different reasons to Carl. I asked why she started using it:
I’ve had a shit life – it numbs all of that. Now being homeless, it helps me to sleep and keeps me warm, but I only use it in the winter because I need to sleep.
In summer, Suzanne explained, she would switch to taking “phet” – amphetamines. I asked her why:
You need to be awake – there are lots of dickheads around. I’ve been beaten and raped in the summer when I was asleep, so you need to be awake more.
Hearing the stories of people fighting their personal battles with mental health and substance use issues was at once haunting and cathartic for me. It was deeply moving to hear them, time and again, struggling with the most difficult aspect of their condition: the simple decision to ask for help. And sadly, far too often, when they did summon the courage, their requests would go unheard, unheeded, or they would be engulfed by a sprawling system that seemed unable to help.
Dave had been using alcohol for many years and had asked for support on several occasions – only to be passed from service to service:
I was made redundant and, at 50, was finding it hard to get another job. I wasn’t drinking all of the time then. But as I started to get into more debt and the bailiffs were knocking on the door, I needed a drink to get me through it. It was not until I was charged with drunk driving that I knew I had a problem.
Dave said he wasn’t shy about asking for help – at least, for a while. But he found himself caught in a downward spiral that led to more drinking, more suffering, and less support:
So many times I’d stop drinking, but I couldn’t deal with the voices in my head. I’d ask for support, but the waiting lists were so long. The medication the doctor gave me did nothing, so I’d start drinking again, and because I’d start to drink again, mental health services wouldn’t touch me. All they kept saying was: ‘You should stop drinking first.’
To expand my understanding, I also sought the perspectives of a dozen people working on the frontline of mental healthcare – from professionals in NHS mental health and substance use teams, to people working for charitable support groups. Their insights revealed a frayed and fragmented network of services, with the holes and inefficiencies obvious and crying out for attention and repair. As one nurse explained:
The stress of trying to get services to help is unbelievable. You’ve got pressure from the person’s family because they are afraid they’ll end up dead. You’ve got pressure from managers to discharge the person. All I’d get is criticism which far outweighed encouragement or support. The stress made me so anxious that I almost gave it all up – and even considered suicide myself.
Over 80% of the professionals I spoke to called for an integration of mental health and substance use teams, in part because of the huge cuts nationwide in funding to substance use services. One social worker in a substance use service explained the current situation:
If you get someone with an alcohol addiction, it becomes quite apparent that they use drink as a way of coping with their mental health. But, because of massive waiting lists within mental health services or because they are told they need to stop drinking before [they can be treated], mental health support can’t be offered. So, the person just keeps drinking and eventually disengages from our services as there is no hope for them. We shouldn’t expect someone to stop using a substance that they perceive is helping without offering an alternative treatment.
For all the professionals I interviewed, the most significant barrier to getting support for someone’s mental health issues was that they used substances and would not receive any treatment until they addressed this. As one mental health nurse told me:
I had one chap who was using cocaine, mainly due to social anxiety. Initially, he’d use it when socialising with friends. But because it gave him confidence and he could talk to people, he started to use it all the time and got himself in debt. I wanted to address the root cause, the social anxiety, so I referred him to our Improving Access to Psychological Therapy service. But I was told he needed to be abstinent from cocaine for three months before they’d accept him. He eventually disengaged, and I haven’t seen him since.

In the shadows of our society, hidden behind the walls of our prisons and in the dark corners of our streets, the experiences of Jenny and countless others bear witness to the profound failings of our healthcare system to address co-existing mental health and substance use issues. For those caught in the merciless cycle of addiction and illness, these systemic inefficiencies and administrative blockades do much to intensify their torment.
Their often brutally honest accounts (and the insights of those who try to support them) draw a portrait of a split and underfunded service, collapsing under the weight of its contradictions. The loud calls for integrated mental health and substance addiction treatment become muffled amid the bureaucratic din of funding cuts, lengthy waiting lists and policy neglect.
The evidence overwhelmingly confirms the need for a model of care that is holistic and integrated – one that shifts the narrative from stigma and isolation to awareness and support.
The economic case for reshaping investment in our mental health and substance misuse services is powerful. The annual cost of mental health problems to the UK economy is a staggering £117.9 billion – equivalent to 5% of its annual GDP![]()
![]()
![]()
![]() – with substance misuse adding a further £20 billion.
– with substance misuse adding a further £20 billion.
However, these figures tell only part of the tale. While we know that 70% of people in treatment for drug misuse and 86%![]()
![]()
![]()
![]() of people in treatment for alcohol misuse have a mental health diagnosis, the full financial impact of people with these co-occurring disorders is probably far greater.
of people in treatment for alcohol misuse have a mental health diagnosis, the full financial impact of people with these co-occurring disorders is probably far greater.
This also includes people who often plough through a punitive and bewildering series of services as they navigate their intersecting problems, encountering barriers at every turn that fail to address their acute health![]()
![]()
![]()
![]() and social care needs. As their distress is amplified, the costs to wider society escalate too – as one social worker explained to me:
and social care needs. As their distress is amplified, the costs to wider society escalate too – as one social worker explained to me:
I am currently supporting a woman who is struggling with alcohol dependency, a condition that began after she endured significant domestic abuse. The cycle is devastating: her trauma cannot be effectively addressed because of her dependency on alcohol, and she cannot abandon alcohol because it’s the only solace she finds from her emotional torment. Despite several attempts at rehabilitation, none of the programmes have sufficiently tackled the mental health aspects of her trauma. Now, with cirrhosis of the liver, her health is in critical decline. It’s a heart-wrenching situation – a stark reminder of the desperate need for integrated treatment approaches that address both substance dependency and the underlying psychological trauma.

In the quiet confines of a West Midlands mental health crisis centre, I’m preparing to meet someone whose story I know only from the clinical notes on my screen. The phrase “is alcohol dependent” is highlighted in bold. Behind those words is another person whose life is unravelling in the silence of a battle fought alone.
John walks into the room, a man living in the grip of two relentless forces – addiction and mental illness. “It was just to stop the noises,” he says of the whisky he uses as medication for his inner turmoil. His hands are trembling. This is the moment of truth – his story is no longer trapped within the clinical pages of a case file.
“I’ve lost everything,” he tells me. “I might as well be dead.”
Then John explains why he’s given up hope:
I’ve asked for help so many times, but all I get told is that I need to stop drinking before my mental health can be treated. However, alcohol is the only thing that works for me. I’ve gone through detox, but then I had to wait months for counselling. I just can’t cope that long without any support – antidepressants don’t do anything for me. What’s the point?
Over the past 15 years, I have met countless “Johns”, both during my day job as a mental health social worker and, latterly, in my academic research. This has led me to conclude that the health and social care system in which I work falls catastrophically short.
This is no mere professional critique. It is an impassioned plea for society to rediscover its collective heart; to explore the human stories that lie hidden in statistics such as that, between 2009 and 2019, 53% of UK suicides were among people with comorbid diagnoses of mental health and substance use.
Instead of viewing people through the limiting lens of labels, we should endeavour to see their humanity. Engaging in conversation, extending empathy and showing compassion are powerful actions. A kind word, an understanding nod or a gesture of support can affirm their dignity and spark a connection that resonates with their innate human spirit. Or as John, whose journey I’ve had the privilege to witness, puts it:
It’s not about the help offered but the meaning behind it. Knowing you’re seen as a person, not just a problem to be solved – that’s what sticks with you.
*All names in this article have been changed to protect the anonymity of the interviewees.
If you or anyone you know require expert advice about the issues raised in this article, the NHS provides this list of local helplines and support organisations.

For you: more from our Insights series:
To hear about new Insights articles, join the hundreds of thousands of people who value The Conversation’s evidence-based news. Subscribe to our newsletter.![]()
Simon Bratt, Mental Health Social Worker and PhD Candidate, Staffordshire University
This article is republished from The Conversation under a Creative Commons license. Read the original article.

A rewarding experience need not be about being in an awesome location. It can be about connecting to where we are, wherever it might be.
Seen in the right way, stumbling along the bank of a stream behind the local supermarket can rival the Inca trail to Machu Picchu.
This is the promise of “drifting”, where we enrich our experience by connecting more fully to our environment through adventurous acts of walking.
It is a practice championed by psychogeographers, who include writers Peter Akroyd, Will Self, Iain Sinclair, and writer and filmmaker John Rogers.
Walking has an enormous power to stir memories of old haunts, as well as trigger new thoughts, feelings, narratives and meanings.
Go your own way
True to its avant-garde roots there are no rules. One early proponent reportedly walked through part of Germany guided by a map of London.
I improvised my own drift on the way to write this by tossing a coin to decide between possible turnings.
But we often don’t need an external input to get ourselves pleasantly lost. We can just go whichever way we are drawn.
Eventually we may start salivating at the path yet to be taken, or cooing over the rusty remains of a Victorian lamppost.
Reading about the areas we walk through can also help send us off in new directions and shed new significance on what we see.

Deepening connection
Drifting grew out of left-wing thought, and a desire to question our relationship with a capital-driven urban environment.
But its psychological effects do not rely on our having specific political outlook. It puts us in the moment, focusing on our our journey not our destination.
And setting out with the attitude that everything is interesting, means we can never be disappointed.
This can all help enrich our relationship with the world outside our door, through our curiosity, interaction and feelings.
My own wandering has has been enhanced by acknowledging it as “a thing” which others do, and have done for generations.
Drifting may never spark a revolution, but it can deliver a reminder that valuable experiences are available to us for nothing. ■
The latest in a series exploring uplifting things to do alcohol-free for no money, having previously looked at improv and cold showers.
{kind=link}